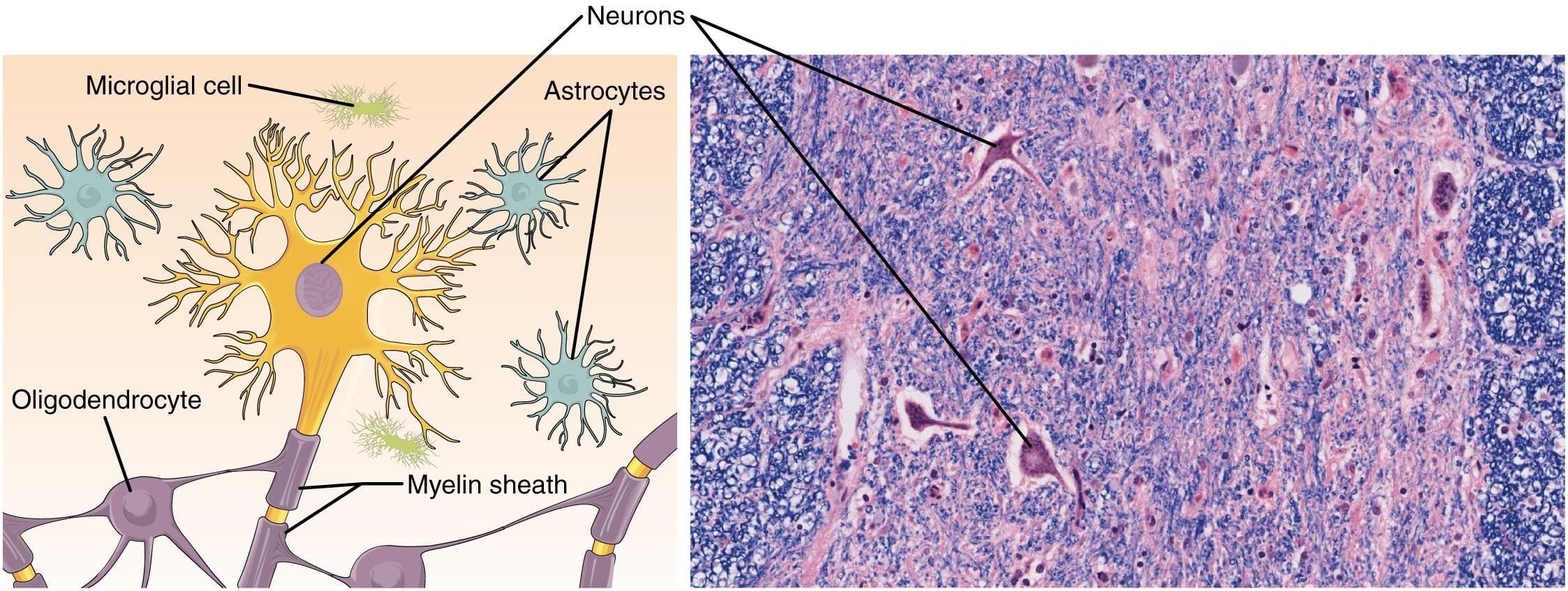
Glial cells
- May be classified as macroglia (which include astrocytes, oligodendrocytes, and ependymal cells) and microglia.
- Provide support and protection for neurons.
- Glial cells outnumber neurons 10 to 1 in the central nervous system.
Astrocytes
- The largest glial cell.
- Support function of neurons in multiple ways:
- Regulates interstitial fluid.
- Modulates signals that regulate blood flow in response to neuronal activity.
- Provides structural support; astrocytes are essential components of the blood-brain barrier and of glial-limiting membranes (aka glial limitans) that line the pia matter and parenchymal vasculature.
- Provides nutritional support via glycogen storage.
- Protects against the death of neurons by activating antioxidant pathways.
Microscopic images of astrocytes

Astrocytes in a Normal Aged Human with GFAP Stain
Medium power microscope slide showing that astrocytes’ cytoplasmic processes are better visualized with special stains like this immunohistochemical stain for glial fibrillary acidic protein (GFAP) which allows one to appreciate their stellate appearance.

Astrocytes in Alzheimer’s Disease Cortex
Medium magnification microscope slide with GFAP stain.

Normal Astrocytes
Astrocytes in gray matter, H&E stain.

Reactive Astrocytes
Astrocytes undergo reactive changes (gliosis). Sometimes they swell with eosinophilic cytoplasm and enlarged nuclei while sometimes, they develop thickened processes creating a pattern of fibrillary gliosis (also called piloid gliosis).

Astrocytes: Normal vs. Reactive vs. Neoplastic
Left: “Resting” astrocyte. Middle: Reactive astrocyte. Right: Neoplastic astrocyte.
Oligodendrocytes
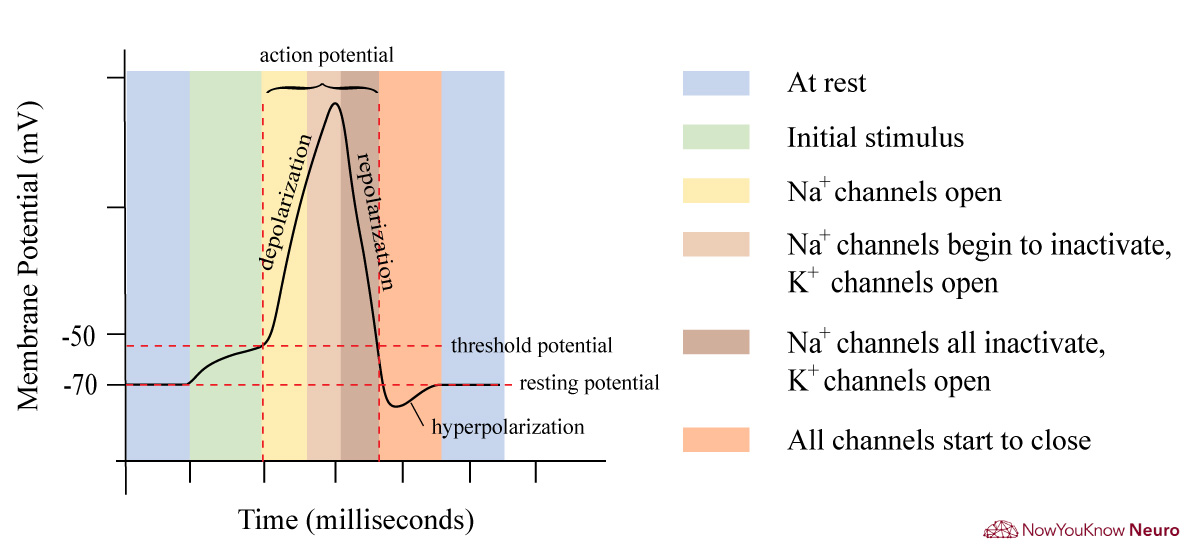
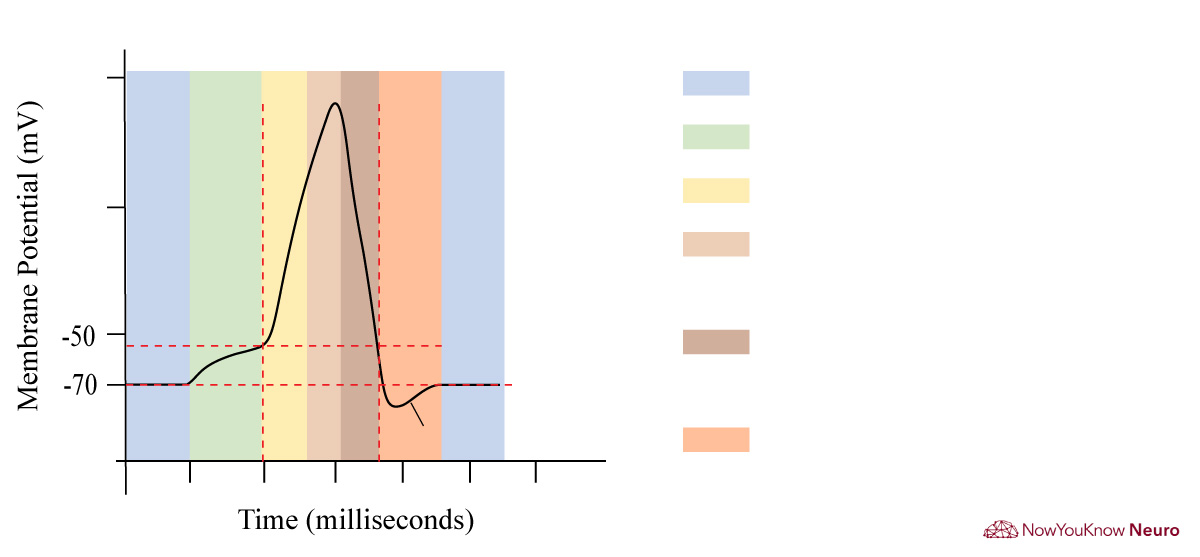
- Responsible for the formation of myelin in the central nervous system
- Myelin provides electrical insulation that allows for saltatory conduction, the speed of which is determined by the length of the internodal myelin segments. Larger axonal diameters conduct faster than smaller diameters.
- Oligodendrocytes have condensed, rounded nuclei and unstained cytoplasm.
Oligodendrocytes vs. Oligodendroglioma

Normal Oligodendrocyte
Oligodendrocyte nuclei can be seen in white matter, often in short chains, and have smaller more dense nuclei than astrocytes.

Oligodendroglioma
Neoplastic oligodendrocytes with rounded nuclei, lacking abundant fibrillary processes, and with perinuclear halos giving it a “fried egg” appearance.

Oligodendroglioma
Neoplastic oligodendrocytes with rounded nuclei, lacking abundant fibrillary processes, and with perinuclear halos giving it a “fried egg” appearance.
Astrocyte-Oligodendrocyte crosstalk
- Communication occurs by direct cell-cell gap junctions, as well as secreted signaling molecules.
- The importance of astrocyte-oligodendrocyte communication is made apparent in primary astrocytopathies such as Alexander disease, and osmotic demyelination syndrome.
Ependymal cells
- Produces and facilitates the movement of cerebrospinal fluid (CSF).
- Lines the ventricles and central canal of the spinal cord.
- Resembles simple cuboidal or columnar epithelium with some cilia and microvilli on histopathology.
Microglia
- The primary immune cell of the central nervous system.
- Responsible for antigen presentation,
- Activates in response to tissue damage and ischemic injury. Once activated, becomes a motile, phagocytic cell (adept for neuronophagia) which forms reactive oxygen species and secretes cytokines and proteases.
- The smallest and rarest glial cell.
- Derived from bone marrow/monocytes and enter the CNS in the perinatal period.
- All other glial cells and neuronal cells are derived from neural tube cells.
Neuronal cells
- Responsible for receiving, integrating, and propagating information to other cells.
- Contains three parts; dendrites, cell body, and axon(s).
- Dendrites
- Receive information from other neurons at synapses.
- Changes in dendritic spines are critical for neural plasticity that occurs during development and learning.
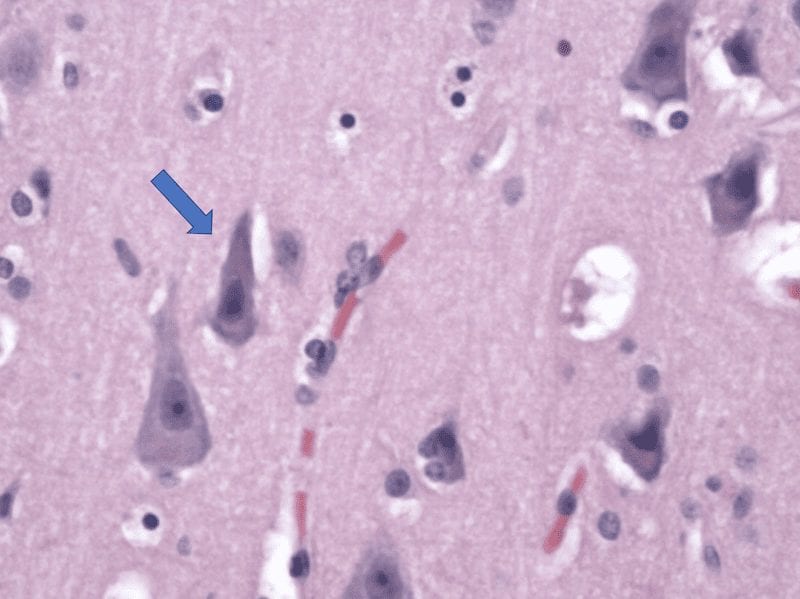
- Cell body
- The main synthetic and trophic center of the cell, it contains the nucleus and most organelles.
- Easily identified by a large central and euchromatic nucleus with a prominent nucleolus.
- Basophilic clumps of polyribosomes are called Nissl bodies.
- Axons
- Conducts information to muscles, glands, or neurons.
- Axons terminate at synapses.
- Dendrites
- There are a few named neurons to be aware of:
- Pyramidal Cells: The prototype cerebral neuron, present in the cortex and hippocampus, with large triangular cell bodies.
- Stellate Cells: Described as GABAergic inhibitory interneurons that control Purkinje cell activity in the cerebellum.
- Purkinje cells: Large distinct neurons in the cerebellum with a prominent pink cell body and extensive dendritic tree.
- These degenerate in various cerebellar degeneration syndromes (e.g. alcohol, chronic phenytoin use, or anti-Yo paraneoplastic syndromes).
- Purkinje cells: Large distinct neurons in the cerebellum with a prominent pink cell body and extensive dendritic tree.
Anatomy of the Neuron
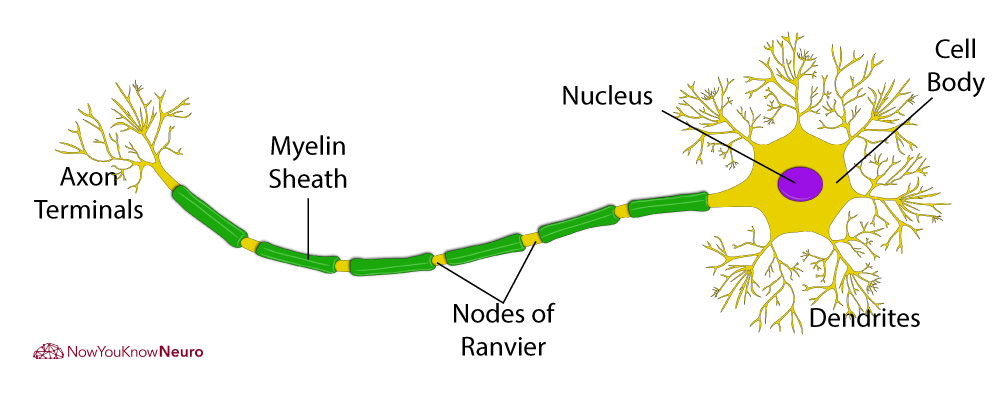
- Most neurons contain multiple dendrites and only one axon.
- Neurons can be easily identified with silver staining on microscopic slides which impregnate neurofilaments.
- Intracellular neurofibrillary tangles can suggest a neurodegenerative disease such as Alzheimer’s disease.
- When the axons of a nerve are severely damaged, Wallerian degeneration occurs.
- Axonal fibers distal to the area of injury degenerate, while proximal fibers survive.