{kind=link}

- Typical findings in CSF include an elevated protein, elevated CSF IgG index, oligoclonal bands in the CSF which do not present in the serum, and possibly slight elevation of WBC count (lymphocytic predominant).
- MRI imaging with contrast is the most important imaging modality in the workup of possible MS.
- Demyelinating lesions related to MS are ovoid, >3 mm in diameter, and are typically located in particular regions: periventricular (Dawson’s fingers), juxtacortical, cortical, or spinal cord.

Multiple Sclerosis Plaque
Pericallosal MS plaque on T2 FLAIR (arrow).

Dawson’s Fingers in Multiple Sclerosis
Sagittal T2 FLAIR MRI.

Dawson’s Fingers in Multiple Sclerosis
MRI T2 flair sequence, sagittal cut.

Multiple Sclerosis Plaques
Axial MRI, T2 FLAIR.
Optic Neuritis (ON)
- Presents with monocular decreased visual acuity, loss of color vision, and an afferent pupillary defect (APD) due to a demyelinating lesion of the optic nerve.
- Pain is also usually present with extraocular movements.
- Children with ON are more likely to present with headache and bilateral symptoms.
- Can be the initial presentation of multiple sclerosis or neuromyelitis optica.
- A funduscopic exam will show a swollen optic disc.
- Optical coherence tomography (OCT) will show thinning of the retinal nerve fiber layer weeks to months after an acute attack.
- Visual evoked potentials (VEPs) of the affected eye will show a prolonged P100 latency, even in patients with distant histories of ON with no residual visual deficits.
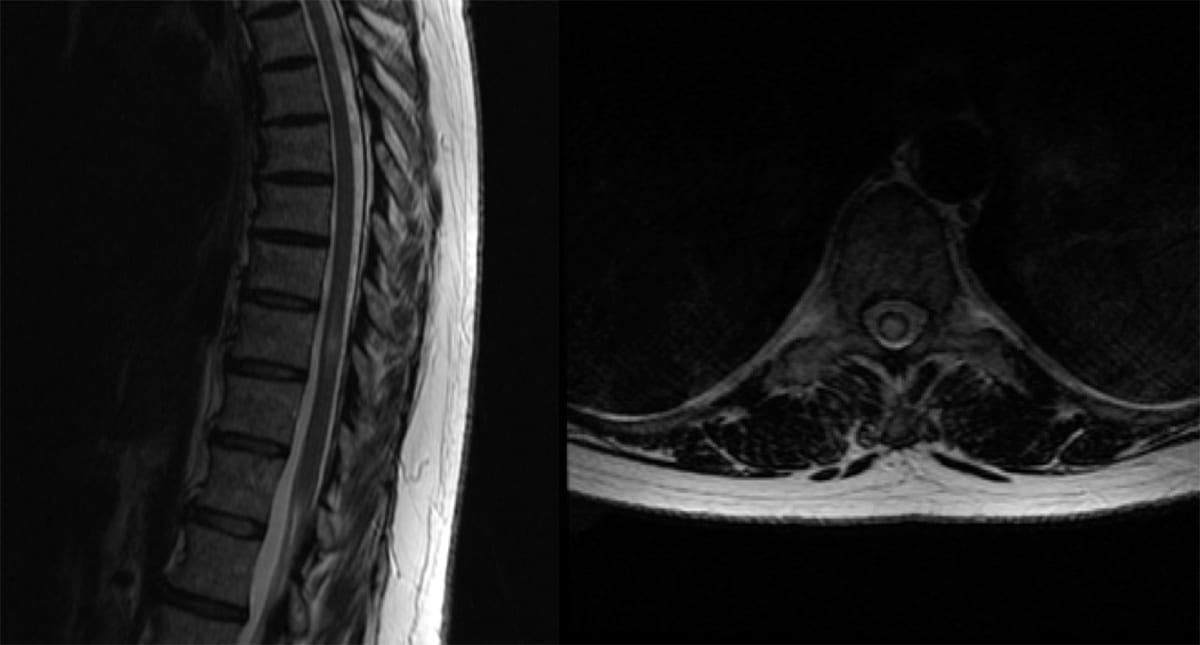
Transverse myelitis (TM)
- Presents with myelopathic findings (weakness, hyperreflexia, sensory symptoms, and occasionally bladder/bowel dysfunction).
- Lhermitte’s sign, an electric shock sensation down the neck/spine with neck flexion or extension) may also be present.
- MRI will show a T2/FLAIR hyperintense lesion involving the spine +/- contrast enhancement based on the lesion’s acuity.
- TM can be the initial presentation of demyelinating disease. However, it is also important to exclude infectious, rheumatologic, postvaccination/postinfectious, and nutritional mimics of demyelinating disease.
- If felt to be truly inflammatory or idiopathic TM once other etiologies are ruled out, then initiation of steroids is indicated.