

The lumbosacral plexus and lower extremity nerves are “high-yield topics” for the boards and in-service examinations. In this chapter, we will discuss the basic physiology and common syndromes of the lumbosacral plexus and lower extremity nerves. One should take time to recognize how these lesions present on the exam as well as with electrodiagnostic testing.
Author: Brian Hanrahan MD
Basics:
Lumbosacral Plexus Diagram
Move the Slider to Practice!
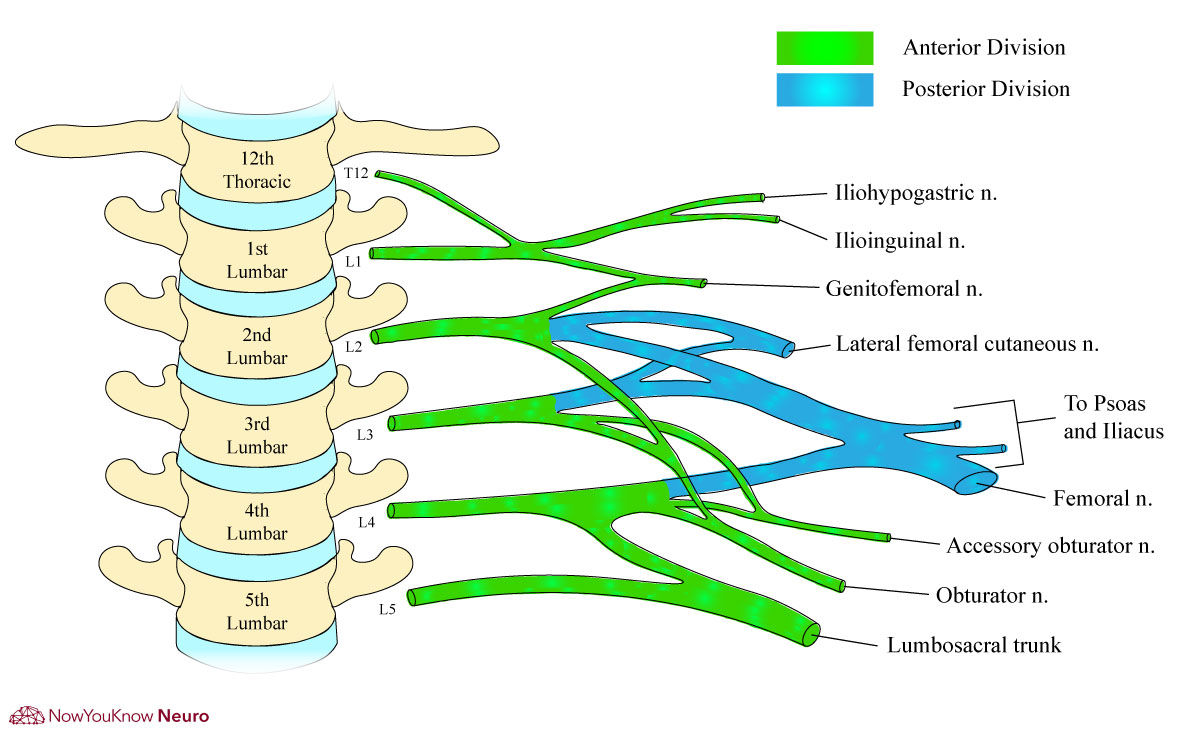
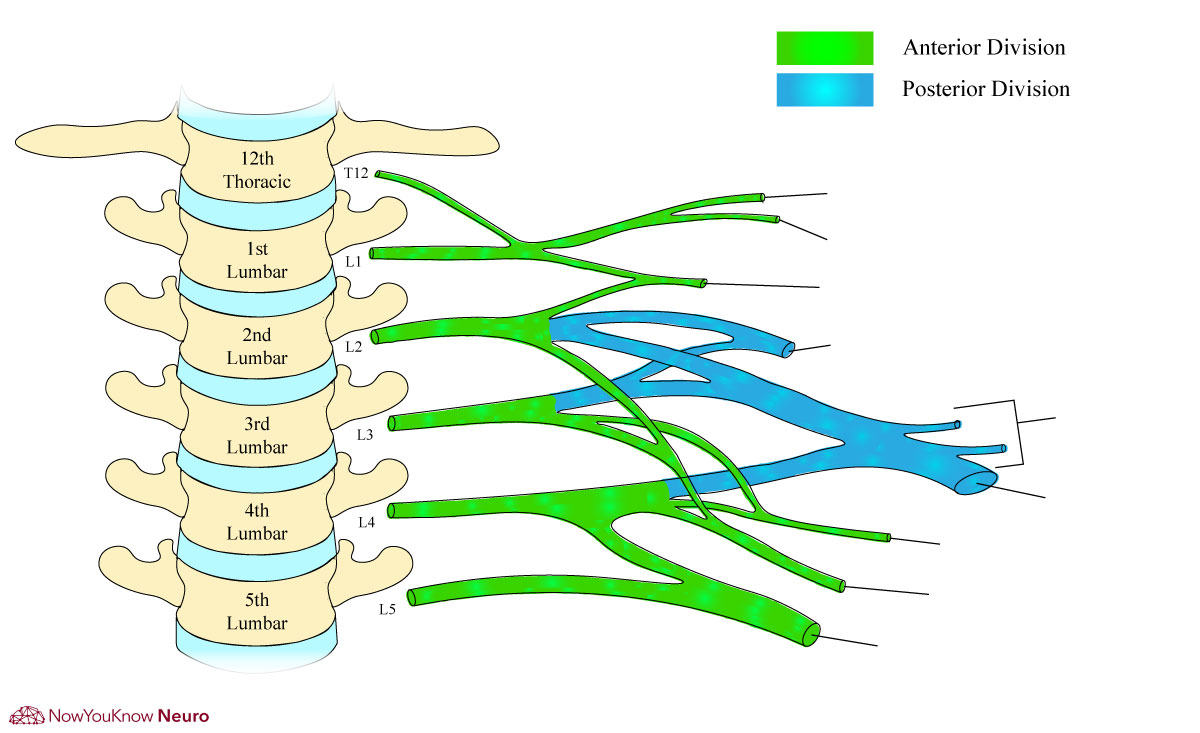
- The lumbosacral plexus is a network of nerve fibers that innervates muscles and provides sensation from the lower limbs.
- It is formed by the anterior rami of T12-L4/5 nerve roots.
- To simplify, the lumbar (T12-L4/5) and sacral plexuses (L4-S4) will be discussed separately.
Table 1: Nerves of lumbar plexus with their associated muscular innervation and function
| Nerve (associated nerve root) | Muscle(s) and function |
| Iliohypogastric nerve (T12-L1) | Internal oblique: Compresses abdominal cavity
Transversus abdominis: Compresses abdominal cavity |
| Ilioinguinal nerve (T12-L1) | Internal oblique: Compresses abdominal cavity
Transversus abdominis: Compresses abdominal cavity |
| Genitofemoral nerve (L1-L2) | Cremaster (males): Raises the scrotum |
| Obturator nerve (L2-L4) | Obturator: Adduction and lateral rotation of hip
Adductor longus: Adduction and flexion of hip Adductor brevis: Adduction and flexion of hip Adductor magnus**: Adduction and flexion of hip Pectineus*: Adduction and flexion of hip Gracilis: Adduction of hip and flexion of knee |
| Femoral nerve (L2-L4) | Iliopsoas: Flexion of hip
Pectineus*: Adduction and flexion of hip Sartorius: Flexion and abduction of hip Quadriceps femoris (rectus femoris, vastus lateralis, vastus intermedius, vastus medialis): Extension of knee. |
*Pectineus is innervated by femoral and obturator nerves, **Adductor magnus is innervated by obturator and sciatic nerves.
Table 2: Nerves of sacral plexus with their associated muscular innervation and function
| Nerve (associated nerve root) | Muscle(s) and function |
| Superior gluteal nerve (L4-S1) | Gluteus medius: Abduction of hip
Gluteus minimus: Abduction of hip Tensor fascia lata: Abduction and medial rotation of hip |
| Inferior gluteal nerve (L5-S2) | Gluteus maximus: Extension of hip |
| Sciatic nerve (L4-S3) | Hamstrings (semitendinosus, semimembranosus: Extension of the hip, flexion of the knee, and rotation of the knee
Adductor magnus**: Adduction and flexion of hip |
| Superficial peroneal nerveª,* (L5-S1) | Peroneus longus: Eversion of ankle (primarily) and assists in plantar flexion
Peroneus brevis: Eversion of ankle (primarily) and assists in plantar flexion |
| Deep peroneal nerveª,* (L4-S1) | Tibialis anterior: Dorsiflexion and inversion of ankle
Extensor digitorum brevis: Extension of toes Extensor digitorum longus: Extension of toes Extensor hollucis longus: Extension of 1st toe and dorsiflexion of ankle Peroneus tertius: Dorsiflexion and eversion of ankle |
| Tibial nerve (L4-S3)ª | Tibialis posterior: Plantar flexion and inversion of ankle
Biceps femoris (long head): Knee flexion Gastrocnemius: Plantar flexion of ankle Soleus: Plantar flexion of ankle Flexor digitorum longus: Plantar flexion of ankle and flexion of 2nd-5th toes Flexor hallucis longus: Plantar flexion of ankle and flexion of 1st toe Abductor hallucis: Abduction and flexion of 1st toe Flexor digitorum brevis: Flexion of 2nd-5th toes Flexor hallucis brevis: Flexion of 1st toe Abductor digiti minimi: Abduction of 5th toe Flexor digiti minimi: Flexion of 5th toe Interossei: Abduction and adduction of toes Adductor hallucis: Adduction of 1st toe Lumbricals III and IV: Flexion of MCP joints and extension of interphalangeal joints |
aTerminal branches of the sciatic nerve, *Terminal branches of the peroneal nerve, **Adductor magnus is innervated by obturator and sciatic nerves, MCP: metacarpophalangeal joint.
Lumbosacral Plexus Syndromes
- Diabetic lumbosacral plexopathy (diabetic amyotrophy):
- Presents with acute back, hip, and buttock pain, followed by bilateral lower extremity proximal and distal weakness.
- It is most commonly observed in patients with well-controlled type 2 diabetes mellitus
- Can also present less commonly in the brachial plexus.
- Recovery takes weeks and can be incomplete.
- It is most commonly observed in patients with well-controlled type 2 diabetes mellitus
- Retroperitoneal hematoma
- Presents secondary to hemorrhage into the psoas or iliacus muscle.
- CT of the abdomen and pelvis is most useful for imaging acute blood in the retroperitoneum.
- Small retroperitoneal hematomas may only compress the femoral nerve, leading to weakness of the iliopsoas and quadriceps muscles.
- Other
- Radiation Plexopathy
- Tumor infiltration/neoplastic plexopathy
- Peripartum plexopathy
Lower Extremity Nerves and Associated Syndromes
Lateral femoral cutaneous nerve (L2-L3)
- Function
- Sensory: Provides sensation to the anterior thigh.
- Associated syndrome(s)
- Meralgia Paresthetica
- Presents with pain in the low back, buttock, anterolateral thigh, and lateral knee
- Often aggravated by standing and relieved by sitting.
- Associated with obesity or pregnancy, and symptoms disappear with weight loss or delivery.
- Meralgia Paresthetica
Obturator Nerve (L2-L4)
- Function:
- Motor: Adduction and flexion of the hip.
- Sensory: Medial thigh.
Femoral nerve (L2-L4)
- Function:
- Motor: Flexion of the hip and extension of the knee.
- Sensory: Anterior and medial thigh (medial cutaneous nerve of the thigh).
- Most common nerve injured during childbirth secondary to direct compression.
Sciatic Nerve (L4-S2)
- The largest peripheral nerve in the human body.
- Provides innervation to the hamstring muscles and adductor magnus before it bifurcates into the common peroneal nerve and tibial nerve.
- Common peroneal nerve (L4-S1)
- May also be called the common fibular nerve.
- Common peroneal mononeuropathy is the most common mononeuropathy of the lower limbs.
- As it travels deep in the thigh it innervates the short head of the biceps femoris.
- Leaving the thigh the common peroneal nerve passes laterally around the fibular head, where it divides into the superficial and deep peroneal nerves.
- Superficial peroneal nerve
- Function
- Motor: Dorsiflexion and eversion of the ankle.
- Sensory: Upper lateral leg.
- Deep peroneal nerve
- Function
- Motor: Dorsiflexion and inversion of the ankle, extension of toes.
- Sensory: Area between 1st and 2nd toes.
- Function
- Function
- Associated syndrome(s)
- Peroneal compression neuropathy at the fibular head
- The most common site of common peroneal injury.
- The superficial position as the peroneal nerve passes the fibular head makes it susceptible to compression.
- Risk factors include significant weight loss and leg crossing.
- Presents with foot drop and “steppage” gait.
- Peroneal compression neuropathy at the fibular head
- May also be called the common fibular nerve.
Tibial nerve (L4-S3)
- The tibial nerve enters the tarsal tunnel behind or inferior to the medial malleolus.
- Function
- Motor: Plantarflexion and inversion of the ankle.
- Sensory: Sole of the foot.
- Associated syndrome(s)
- Tarsal Tunnel Syndrome
- Occurs due to entrapment of the distal branch of the tibial nerve at the medial ankle (the medial plantar nerve).
- Presents with pain and paresthesias around the medial malleolus
- Pain is often worse at night and with weight-bearing.
- Causes include trauma, degenerative bone disease, and rarely, mass lesions.
- Tarsal Tunnel Syndrome
Sural nerve (S1)
- Formed by the coalescence of distal branches from the tibial and peroneal nerves.
- Function:
- Sensory: Lower posterior/lateral leg, lateral ankle, and lateral foot.
Log in to View the Remaining 60-90% of Page Content!
New here? Get started!
(Or, click here to learn about our institution/group pricing)1 Month Plan
Full Access Subscription
$142.49
$
94
99
1 Month -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
3 Month Plan
Full Access Subscription
$224.98
$
144
97
3 Months -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
1 Year Plan
Full Access Subscription
$538.47
$
338
98
1 Year -
Access to full question bank
-
Access to all flashcards
-
Access to all chapters & site content
Popular
Loading table of contents...
Loading table of contents...