

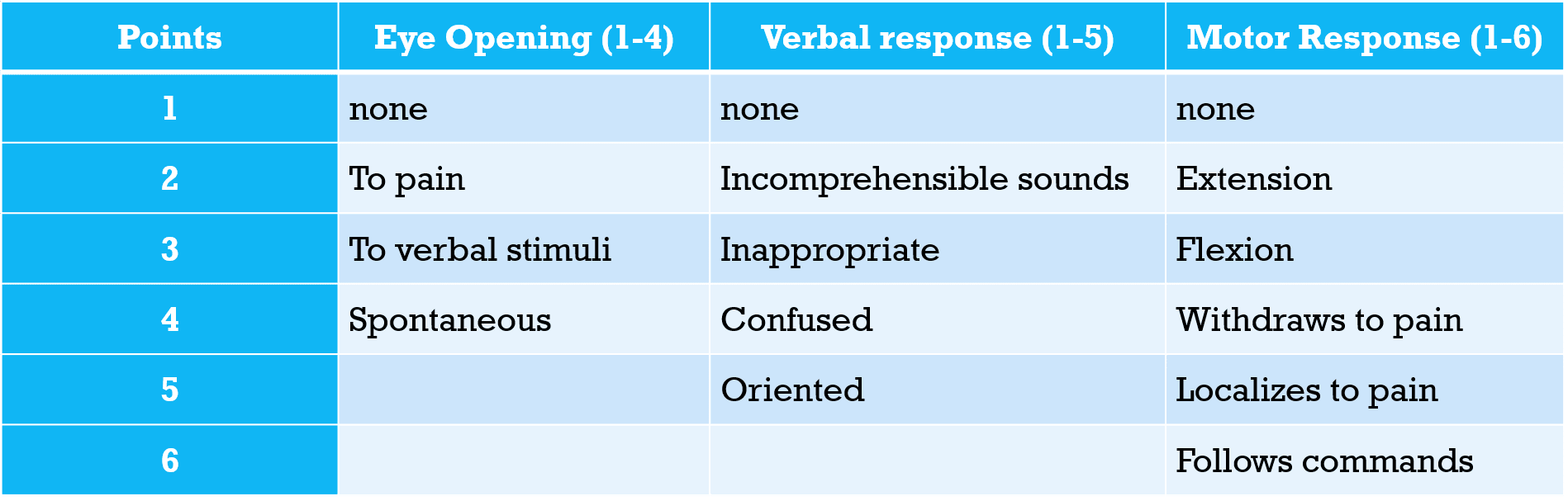
Glasgow Coma Scale (GCS)
- GCS ranges from 3 (profoundly comatose) to 15 (normal).
- Common causes of TBI include falls, motor vehicle accidents, assaults, explosive blasts, and penetrating injuries.
- The more severe the TBI, the higher the risk for the development of focal epilepsy.
- Radiographic findings consistent with TBI:
- Skull fractures
- Cerebral contusions, typically in areas where brain parenchyma rubs against skull bone (i.e. inferior temporal and frontal lobes)
- Coup contusions occur on the side of the trauma.
- Countercoup contusions occur on the opposite side of the site of impact.
- Pneumocephalus due to penetrating injury or skull fracture.
- Can be associated with pneumolabrinth (air in the inner ear).
- Cerebra edema

Acute Brain Contusion

Contrecoup Contusion

Old Inferior Frontal Lobe Contusions

Cerebral Contusion
Axial CT head.
Diffuse axonal injury
- Due to shearing forces from extreme acceleration and deceleration.
- A biopsy will have swollen proximal ends of axons in the appearance of bulbs known as “retraction balls.” Punctate hemorrhages may also be seen.
Basilar skull fracture
- Battle’s sign (ecchymosis of the mastoid region) and raccoon eyes (periorbital ecchymosis) may be seen.
- May also have leakage of CSF from the ears (otorrhea) or nose (rhinorrhea).
- Can test rhinorrhea or otorrhea for β-transferrin, to determine if a CSF leak is present, as this is only positive in CSF.
Non-accidental trauma in a child
- Suspicious signs include spiral fracture of the humerus, immersion burns, rib fractures, retinal hemorrhages (from shaking), long bone injuries, duodenal hematomas, brain contusions, subdural hematoma, and skull fracture.